
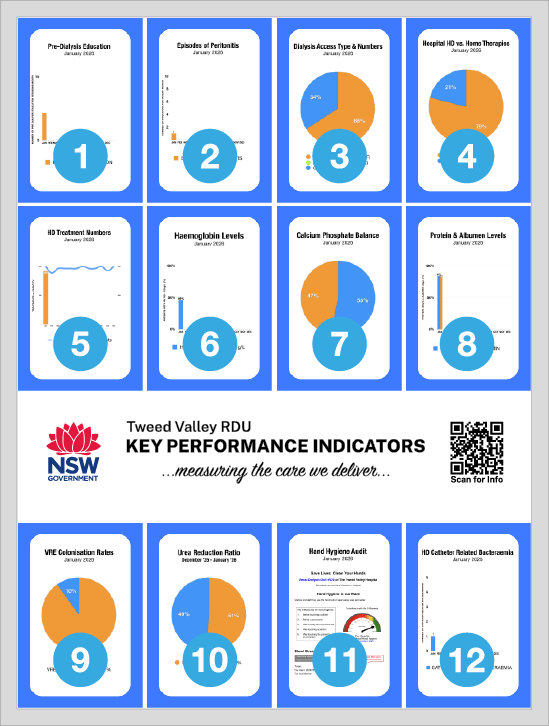
What is a KPI?
Key Performance Indicators (or “KPI’s”) are a way of measuring the effectiveness of the care we deliver. At the Tweed RDU, 11 KPI’s have been chosen to keep track of our practices. The Tweed RDU KPI’s can also be compared to results obtained by similar sized renal units throughout Australia using the yearly “ANZDATA” survey.
1. Pre-Dialysis Education
Pre-dialysis education includes information about renal disease, along with advice about the different types of dialysis, diet and medications. Educating pre-dialysis patients is one of the major functions of the Renal Outreach Department. Research shows that educating patients with renal failure before they need to commence dialysis is a useful and important way of slowing the progression of kidney disease, and also appears to delay the start of dialysis in patients with end stage renal failure7.
2. Episodes of Peritonitis
Peritonitis is the leading complication of Peritoneal Dialysis (PD), a potentially life threatening occurrence, and the major cause of PD failure6. PD associated peritonitis is caused by bacteria infecting the peritoneal cavity during the dialysis procedure. This KPI outlines the rate of peritonitis in patients undergoing peritoneal dialysis.
3. Type of Access
Research states1 that the best access for haemodialysis is the arterio-venous fistula (AVF). When a AVF is not possible, the next best option is a arterio-venous graft (or AVG). Cuffed tunnelled central venous catheters (“Perm-caths”) should only be used if there is no other option for haemodialysis. Our goal is to have most of our patients with a functioning AVF or AVG, and to use catheters for haemodialysis only when necessary.
4. Hospital Dialysis vs. Home Therapy
The number of patients we care for, and the ratio of patients receiving “Hospital” compared to “Home” dialysis therapies is an important KPI. NSW Health has set Tweed Heads RDU the goal of having greater than 50% of patients we care for on some form of Home Dialysis therapy.
Are you interested in “Home” dialysis?
Discuss your options with your Primary Nurse, or with one of the Nephrologists during your next clinic.
5. HD Treatment Numbers
This graph lists the number of haemodialysis treatments we perform each month. Also on the graph is the current funded capacity of our RDU.
6. Haemoglobin
Haemoglobin (Hb) is a protein found in the red cells in your blood. Your Hb level is checked every month in your routine dialysis pathology. The main function of haemoglobin is to carry oxygen from your lungs to your body, a process which is essential to life. Most red cells are made in the bone marrow. A hormone called erythropoietin (EPO), made in your kidneys, signals your bone marrow to make new red blood cells. When you develop kidney failure, you lose the ability to make EPO. As a consequence, many patients with renal failure become anaemic. Most people with renal failure need injections of a synthetic EPO, prescribed by your Nephrologist, so that your body continues to produce red cells. The ideal Hb range for dialysis patients is 105 - 120 g/L.
How can I maintain a healthy Hb?
Kidney disease limits your body’s ability to absorb iron from the gut, resulting in iron deficiency. So in addition to regular synthetic EPO prescribed by your Nephrologist, anaemia caused by dietary deficiency can be prevented by having a balanced diet. Supplemental iron can be given in the form of tablets or injections.
7. Calcium Phosphate Balance
The Calcium-Phosphate Product (Ca x PO4) is calculated by multiplying your Calcium level by your Phosphate level. There is evidence4 to suggest that a Ca x PO4 over 4.0 mmol/L is associated with increased rates of heart disease and death in Haemodialysis patients.
How can I reduce my Ca x PO4?
There are a couple of things you can do to reduce your Ca x PO4. First, make sure you avoid eating foods that are high in Phosphate. Next, make sure you take your Phosphate binder medications exactly as your Nephrologist has prescribed them. Also, make sure you don’t cut your dialysis time short or skip dialysis sessions.
Need more advice? Speak to your Primary Nurse or one of the Nephrologists.
8. Protein & Albumin
Protein is a fundamental component of all living cells. It is essential for the growth and maintenance of body tissues, fighting infection and wound healing. Protein is also involved in transporting cholesterol and fat soluble vitamins. Albumin is the most abundant protein found in the blood. Low Albumin levels are frequently found in dialysis patients, and low albumin levels are directly related to increased rates of illness and death in dialysis patients5.
9. VRE Colonisation
Enterococci are harmless germs which live in your intestines. Vancomycin is an antibiotic that is often used to treat very serious infections. Vancomycin Resistant Enterococci (VRE) is a germ that has become resistant to, and cannot be destroyed by, Vancomycin. You are checked for VRE every third month when your Primary Nurse gives you a container (“Poo Pot”) for a faeces sample.
How can I avoid catching VRE?
The most common way VRE is spread is by touching someone who is colonised or infected. Touching a surface, such as a hospital bed or table, that has the bacteria on it can also spread VRE. The most important thing you can do is to regularly and thoroughly wash your hands3, particularly after going to the toilet. Health workers treating you should wash their hands each time they enter and leave your room, and before and after performing any procedure. This will kill the VRE and stop it from spreading to others.
10. Urea Reduction Ration
The “Urea Reduction Ratio”, or URR, is a method of measuring the efficiency of haemodialysis. It is calculated by measuring the urea levels in your blood before and after a haemodialysis treatment.
How can I improve my URR?
If your URR is persistently low, there are several ways to improve it. One way is to increase the time you spend on dialysis. Home HD is the best way of achieving this. It is very unusual to have a home HD patient with a poor URR. You may also need a larger haemodialysis filter. Sometimes a poor URR results from a poorly functioning vascular access. You may also be able to increase the speed of the dialysis pump. The final method of increasing your URR is to have more frequent dialysis sessions.
11. Hand Hygiene Audit Results
There is a simple way to reduce the transmission of infections in hospitals: wash your hands! Staff are audited randomly and regularly throughout the year by Hand Hygiene Auditors. Auditors focus on the "5 Moments" of Hand Hygiene:
1. Before touching a patient
2. Before a procedure
3. After a body fluid exposure risk
4. After touching a patient
5. After touching the patient's environment
This graph is updated every quarter when the audit results are published.
12. HD Catheter Related Bacteraemia
Infections that are related to a patient’s dialysis access are potentially life threatening2. This KPI outlines the rate of infections of the blood (bacteraemia) in our haemodialysis (HD) patients.
How can I reduce my chances of getting an access infection?
The most important way to prevent the spread of infection is to wash your hands! You should wash your hands when you arrive in the RDU, and patients with AVF’s and AVG’s should wash the skin over their access with soap and water before sitting down.
If you have a catheter, make sure you keep the dressing dry. Your central venous catheter dressing will be changed every 7 days, and more often if it is coming off or soiled. PD catheter site dressings should be changed following the advice of your PD Nurse.
Ask your Primary Nurse if you need more information.
References
- Hodges TC, Filinger MF, Zwolak RM, et al: Longitudinal comparison of dialysis access methods: risk factors for failure. J Vas Surg 1997; 26:1009
- Hoen B, Kessler M, Hestin D, Mayeux D: Risk factors for bacterial infections in chronic haemodialysis adult patients: A multicentre prospective survey. Nephrol Dial Transplant 10:377-381, 1995.
- Duval, Linda: Infection Control 101. Nephrology Nursing Journal 37, 485-488, September/October 2010.
- Block GA, Hulbert-Shearon TE, Levin NW, Port FK: Association of serum phosphorus and calcium x phosphate product with mortality risk in chronic hemodialysis patients: a national study. Am J Kidney Dis 31:607-617, 1998.
- George A Kaysen, Vijay Rathore, Gregory C Shearer and Thomas A Depner: Mechanisms of hypoalbuminemia in hemodialysis patients. Kidney International 48, 510–516, 1995.
- Piraino, B, et al: Peritoneal dialysis related infection recommendations: 2005 update. Peritoneal Dialysis International 2005; 25:107-131.
- Thomas, M.: Pre-dialysis education for patients with chronic kidney disease. Nephrology 2007; 12, 46-48.

©2026